Diabetic foot ulcers (DFUs) are one of the most serious and least-talked-about complications of diabetes. They affect up to 34% of people living with diabetes, carry a 40% recurrence rate within a single year, and are a leading cause of non-traumatic limb amputation worldwide. Despite decades of medical advancement, standard treatments — wound dressings, antibiotics, and surgical debridement — still fail a significant number of patients.
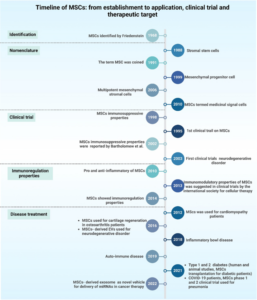
That’s why scientists are turning to regenerative medicine, and specifically to a type of adult stem cell called mesenchymal stem cells (MSCs), as a potential game-changer. A comprehensive review published in the World Journal of Diabetes (PMC10704202) explores not just whether MSCs can help heal diabetic foot ulcers, but — critically — how to deliver them effectively to get the best results.
Why Diabetic Foot Ulcers Are So Hard to Heal
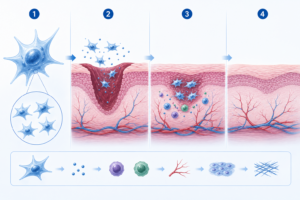
To understand why DFUs are so difficult to treat, it helps to know how normal wound healing works. Healthy wounds close through four overlapping phases: stopping the bleeding (hemostasis), fighting infection (inflammation), rebuilding tissue (proliferation), and remodeling the scar (maturation). In people with diabetes, this process is disrupted at almost every stage.
High blood sugar causes poor circulation, which starves the wound of oxygen and nutrients. Nerve damage (neuropathy) means patients often can’t feel the wound worsening. Chronic inflammation prevents the healing process from progressing. Oxidative stress damages cells before they can repair tissue. The result is a wound that simply stalls — unable to close, vulnerable to infection, and at constant risk of becoming life-threatening.
What Are Mesenchymal Stem Cells?
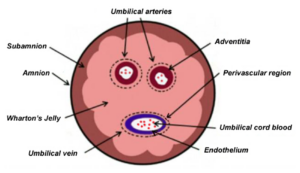
Mesenchymal stem cells are adult stem cells found naturally in bone marrow, fat tissue, the umbilical cord, and other parts of the body. Unlike embryonic stem cells, they carry no ethical controversy, are relatively easy to harvest and grow in the lab, and have a strong safety track record in clinical research.
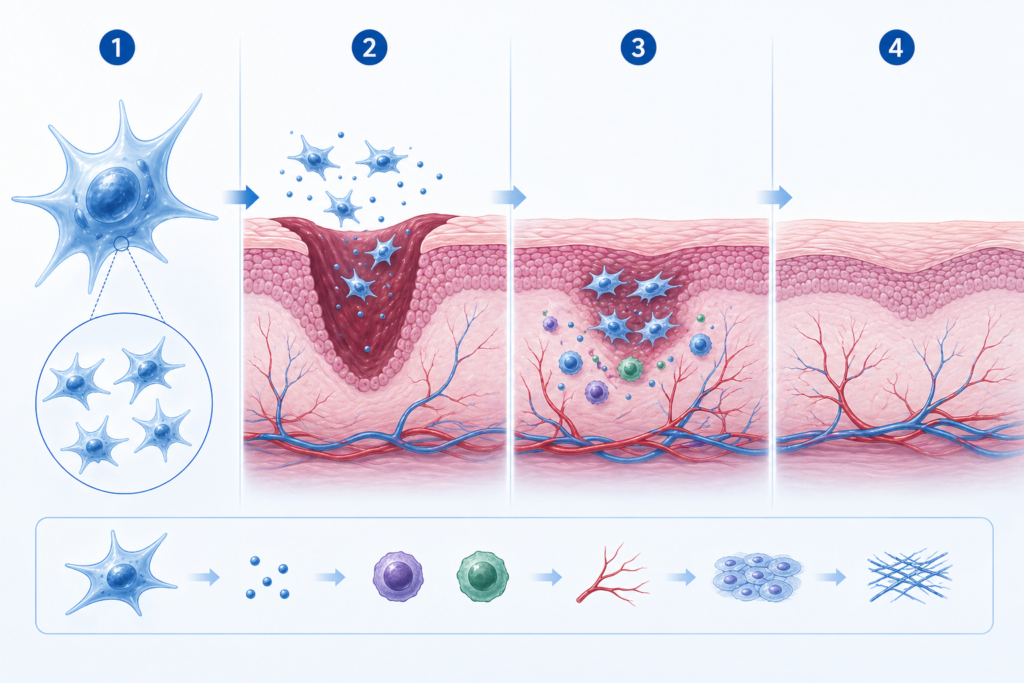
MSCs help wounds heal in two key ways. First, they can directly differentiate — that is, transform themselves into the specific cell types a wound needs, such as fibroblasts that lay down connective tissue, endothelial cells that build new blood vessel walls, and myofibroblasts that physically contract and close the wound.
Second, and perhaps more importantly, MSCs work through paracrine signaling — releasing a cocktail of growth factors and cytokines that signal surrounding cells to grow, migrate, and repair. Key molecules released by MSCs include VEGF (vascular endothelial growth factor, which drives new blood vessel formation), EGF (epidermal growth factor), bFGF, and IGF-1, among others. In diabetic wounds where blood vessel growth is severely impaired, this ability to stimulate angiogenesis is particularly valuable.
The Problem: MSCs Don’t Survive Long Enough
Here’s where the challenge lies. When MSCs are simply injected into a wound, most of them die within hours or days. The hostile diabetic wound environment — low oxygen, high glucose, intense inflammation — is toxic to the transplanted cells. Those that survive tend to migrate away from the site. As a result, the therapeutic benefit is short-lived and inconsistent.
This is the central problem the review article sets out to solve: not whether MSCs work, but how to keep them alive and active at the wound site long enough to make a real difference.
The Role of Exosomes: Healing Without the Cell
Before exploring delivery solutions, the research highlights a fascinating discovery that is reshaping the field. Much of the healing benefit from MSCs doesn’t actually come from the cells themselves — it comes from tiny particles the cells release called exosomes.
Exosomes are nanoscale biological “packets” that MSCs secrete as part of normal cell communication. They carry microRNAs, proteins, and other signaling molecules that instruct nearby cells to reduce inflammation, grow new blood vessels, deposit collagen, and regenerate skin. Studies cited in the review showed that MSC-derived exosomes reduced wound inflammation, improved blood vessel formation, and accelerated wound closure in diabetic animal models.
What makes exosomes especially exciting is their practical advantages over live cells: they are more stable, can be stored more easily, have a lower risk of immune rejection, and sidestep many of the safety concerns associated with transplanting living cells. Researchers now see exosomes — particularly when paired with smart delivery systems — as the next frontier in DFU therapy.
Four Delivery Systems That Could Change Everything
The core of the review examines four types of scaffold-based delivery systems designed to support MSCs (and their exosomes) at the wound site, improving their survival, retention, and therapeutic effect.
Hydrogel Scaffolds are water-absorbing polymer networks that mimic the moist, gel-like environment of natural tissue. They protect MSCs from the harsh wound environment, maintain moisture (critical for wound healing), and can be engineered to release cells and growth factors slowly over time. Natural hydrogels made from collagen or hyaluronic acid are highly biocompatible; synthetic options offer greater mechanical strength. Hybrid designs are increasingly combining the best of both. Research has shown that MSCs delivered via hydrogels have significantly better survival rates and produce stronger healing outcomes than injected cells alone.
Fiber Scaffolds, produced by a process called electrospinning, are three-dimensional meshes of microscopic or nanoscopic fibers. Their structure closely resembles the natural fibrous architecture of human tissue, making them an excellent surface for cells to attach and grow. They have been used successfully in skin, bone, vascular, and neural tissue engineering, and studies show they can effectively support MSC activity in diabetic wound models.
Sponge Scaffolds are highly porous, three-dimensional structures created by freeze-drying or gas foaming techniques. Their interconnected pore networks allow oxygen, nutrients, and cells to flow freely throughout the material. The right pore size — generally in the range of a few hundred microns — is key to ensuring cells remain viable and active. Multiple studies demonstrated that MSCs in sponge scaffolds reduced inflammation, boosted anti-inflammatory signaling, promoted new blood vessel growth, and significantly accelerated wound closure in diabetic animal models.
Acellular Bioscaffolds are perhaps the most biologically sophisticated option. They are created by taking real tissue from human or animal donors and chemically, mechanically, or enzymatically removing all the living cells — leaving behind only the extracellular matrix (ECM). This natural scaffold is rich in collagen, elastin, fibronectin, and laminin, providing an almost ideal biological environment for MSCs to thrive. The trade-off is that the decellularization process is complex and time-consuming, but results in preclinical studies have been compelling.
What Does This Mean for Patients?
The honest answer is: we’re not there yet, but the direction is clear and encouraging. Preclinical studies — primarily in animal models — have produced impressive results across all four delivery systems. MSCs supported by these scaffolds consistently outperformed unsupported MSC injections in terms of wound closure speed, tissue regeneration, and reduction of inflammation.
However, the review’s authors are candid about the limitations. Clinical data in humans remains limited, and results from animal studies don’t always translate directly to human patients. More rigorous clinical trials are needed before any of these approaches can become standard care. Questions around long-term safety, scalability, cost, and manufacturing consistency also need to be resolved.
The Bigger Picture
What this research represents is a fundamental shift in thinking about regenerative wound care. The question is no longer simply “can stem cells help?” — the evidence strongly suggests they can. The question is “how do we engineer the right environment to let them do their job?”
The combination of MSC-derived exosomes with smart, biomimetic delivery platforms like injectable hydrogels is emerging as the most promising direction. As materials science, cell biology, and clinical medicine continue to converge, treatments that once seemed futuristic — using the body’s own cellular machinery, delivered precisely and effectively to a chronic wound — are moving steadily closer to reality.
For the millions of people living with diabetes who are at risk of DFU, that progress can’t come soon enough.